
Last year, during his final semester of medical school, Eric Macaluso, DO, spent a month in two of the starkest and most remote corners of the United States.
Macaluso, 26, practiced building a temporary shelter, studied how to identify signs of frostbite, and climbed through the snowy woods at Colorado’s Breckenridge Outdoor Education Center (BOEC) to study avalanches. Under the guidance of faculty from BOEC and Thomas Jefferson University’s Sidney Kimmel Medical College (SKMC) in Philadelphia, he learned about hypothermia, plant toxicology, and navigating with the help of the night sky, and participated in a mock nighttime rescue operation. He also canoed down the Green River in Colorado and hiked through 20 miles of Utah desert — all as part of a wilderness medicine course that teaches medical students how to rescue, triage, and treat patients in intensely punishing conditions.
Macaluso, now a first-year family medicine resident at Crozer-Chester Medical Center in Upland, Pennsylvania, certainly appreciated the insight he gained into wilderness medicine, a subspecialty of emergency medicine. But he deeply valued the opportunity to assume more responsibility than he might typically have otherwise.
“It was very powerful to get to practice taking the lead in medical care in some extremely stressful, though simulated situations,” he says. “This was one of the most meaningful experiences I had during all of med school.”
Every year thousands of future physicians like Macaluso participate in what are known as away rotations — educational experiences that take them far beyond the walls of their home institutions.
Sometimes their aim is to “audition” for a residency program they hope to attend or to earn a letter of recommendation to increase their odds in the competitive residency application process. They may also opt for away rotations to gain training not offered at their home institution or to confirm budding interest in a particular specialty. And all DO candidates are required to complete an away rotation in order to graduate.
But sometimes away rotations are a chance to dip into the extraordinary.
More unusual electives take students on ambulance rides, into autopsy suites, behind the walls of prisons, or into a professional kitchen to study culinary medicine. Students can even experience zero gravity during an aerospace medicine clerkship run by NASA.
Often, the journey begins with a search through the AAMC Visiting Student Learning Opportunities™ (VSLO®) database. There, students can find more than 15,000 opportunities at hundreds of institutions. Users can search by desired specialty, institution, and such factors as duration — usually four weeks — and tuition-free offerings.
Each host institution sets its own application requirements, but they often include transcripts, letters of recommendation, and personal statements — all of which get uploaded via the VSLO application platform. Although the service is open year-round, most students apply in March.
Often, these electives not only help students with the residency application process but are also highly valuable educational experiences, says Robin Carle, senior director of the VSLO program. “Away rotations offer opportunities that students may never be able to replicate once they move into residency and their careers.”
Here are four away rotations that help participants hone some highly unique skills — plus cultivate talents that are crucial no matter how these future doctors end up providing care, performing research, or otherwise serving patients.
Cutting-edge transplants

“It’s amazing,” says surgeon Garrett Roll, MD, of the dramatic recoveries made possible by organ transplantation.
“You can see a patient, a person who had needed dialysis for a decade, produce urine for the first time right on the operating table,” says Roll, who teaches a four-week transplant clerkship at the University of California, San Francisco (UCSF) School of Medicine. “You can see someone who was on the verge of death walk out of the hospital on their way to being healthy again a week or two later.”
Each year some two dozen medical students get to experience those life-changing moments up close.
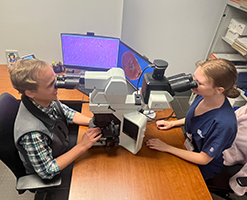
Trainees are intricately involved throughout, beginning with identifying potential organ recipients — a process that entails the ethical allocation of a scarce and precious resource. Students can also scrub in during the several transplant surgeries performed by UCSF physicians each week. And after surgery, students join a multidisciplinary team of providers — from hepatologists to pharmacists to social workers — who collaborate to care for patients adjusting to their new pancreas, liver, or kidney.
Rashmi Bharadwaj, a University of Kentucky College of Medicine fourth-year student who attended the training in October, points to a particularly powerful experience: joining a late-night organ-procurement trip.
“I felt so lucky to be part of the retrieval procedure, which most medical students never even see. I also got to play a small role in preparing a liver for transport to the recipient,” says Bharadwaj, who is applying to residency in general surgery. “It was definitely a highlight of medical school for me.”
At UCSF, providers have the ability to access cutting-edge technologies that better preserve organs during transport. “Usually they just go into a cooler, but we are able to connect organs to a perfusion machine that pumps blood through the organ,” says Roll. “Basically, the technology is tricking the organ into thinking it’s still inside a body.”
Students also get to witness live-donor surgeries, Roll adds. “These can be pretty exquisite technically. Removing part of a donor’s liver needs to be done perfectly to make sure the donor has an uneventful recovery,” he says.
Bharadwaj valued the exposure to such specialized techniques, but she appreciated the patient-care side of transplantation even more.
“It was so nice that we had a moment of silence to honor the deceased donor. It was important to really understand what was happening here,” she notes. “Someone had lost their life, but they were trying to give life to others.”
She also appreciated the opportunity to connect with organ recipients. “I got to be part of life-changing moments,” she adds. “That felt like such a privilege. I will never forget those patients.”
Eye-opening ambulance rides

When an ambulance team heads out on a call, first responders never know exactly what awaits.
They may find a woman in labor, a baby in cardiac distress, a driver thrown from a car, or a patient suffering from a psychotic episode, says David Wampler, PhD, a professor in the UT Health San Antonio Department of Emergency Health Services.
“Paramedics may have to act like a cardiologist, pulmonologist, or trauma surgeon. They have to be prepared for anything.”
And during a four-week rotation spent on board San Antonio Fire Department ambulances, so do dozens of medical students each year.
Students head out on shifts usually lasting eight hours where, under the supervision of seasoned paramedics, they can practice a number of procedures they may not get to perform during other rotations.
Wampler works to ensure trainees are ready for the challenge. For one, all participants must be fourth-year students and have already completed basic life support training. Then Wampler covers topics ranging from how to ride safely in an ambulance to the skills for managing mass-casualty events.
“Often, as students, we’re involved more on the patient-management side, like taking a history, but this rotation was tremendously hands-on,” says Chloe Busse, a fourth-year student at the New York Institute of Technology College of Osteopathic Medicine at Arkansas State University who plans to study emergency medicine. “Here we had many more opportunities to start IVs, hook up EKGs, and intubate patients. We could do pretty much anything the paramedics could do.”
Busse also appreciated the chance to better understand patient handoffs. “I got to learn how much detail ED staff really need as we are transferring someone to their care.”
Of all the experiences available to students during the rotation, Wampler considers the opportunity to see inside patients’ homes one the most impactful.
“In medical school we talk about social determinants of health. But in Emergency Medical Services you get to see, taste, and smell them,” he says. “Seeing the home can explain why a patient might get a postoperative infection or may not take their medications. It provides incredible insights.”
Busse highlights the deeply human side of treating patients in crisis as well.
She describes one woman she met during a late-night ambulance ride in January. “It looked like she had taken a lot of pills, and we were concerned she was overdosing. She was a bit resistant and belligerent.”
But Busse was able to connect in a personal way. “She was complaining that her hair was too messy, and I agreed to braid it for her. It was a simple gesture, but it made her feel good. We got to the hospital and she said, ‘Thank you so much,’” Busse recalls.
“That’s what I love about medicine — the chance to be a compassionate heart and a helping hand in a time of tremendous distress.”
Inside an autopsy
Autopsies aren’t so much about deceased people — they’re very much about the living. That’s a key principle behind the work of Justin Rueckert, DO, director of an autopsy-related rotation at the University of Kentucky College of Medicine (UKCOM) in Lexington.
“Sometimes people request an autopsy to help them feel they have every piece of information possible [about their deceased loved one]. It can help them move on,” he explains.
Autopsies are also about future patients who will benefit from the scientific knowledge hidden within a decedent’s tissues. “A family may request an autopsy for purely altruistic reasons, like if their relative had a rare disease,” he says.
And autopsies are highly valuable to the medical students who participate in the four-week autopsy rotations that UKCOM offers 10 times annually, Rueckert adds.
In fact, the learning starts before students ever enter the autopsy suite. Often, the first step is to observe phone calls to families seeking permission in cases when the hospital or provider requests the autopsy.
“We are calling people on one of the worst days of their lives. Students get to hear how we navigate very challenging conversations,” says Rueckert. “If a family gets upset, I advise students to remember that it isn’t personal. It’s just about the grieving process.”
Next, trainees begin practicing the many technical skills necessary to assess a cadaver. They may inspect wounds, search for signs of infection, and obtain tissue to later examine under the microscope. But even more valuable, Rueckert says, is the opportunity to hold a diseased organ in their own hands.
“If you hold a cirrhotic liver, you can feel the firmness from all the scar tissue,” he says. “Working in the autopsy suite is a walk through a pathology textbook. It’s a fantastic teaching platform for disease processes, no matter what field a student ultimately enters.”
The lessons extend even further, says Rueckert, onto a societal plane.
“What I love most about working with medical students is helping them see the importance of determining the cause of death. If a cause of death declaration is incorrect — which happens often — then national mortality statistics will be incorrect too.
“I want students to know that the cause of death statements they’ll write in the future will have major implications. Mortality statistics drive so much — health care policy, research, community initiatives,” he says. “If the input is flawed, then those outputs will be flawed as well.”
Into the wild
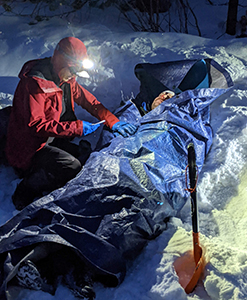
On one night during the wilderness medicine rotation run by Thomas Jefferson University’s SKMC, students head out for a highly realistic simulation of an airplane crash. The rescue assignment usually takes seven grueling hours.
Participants — generally 15 students — set up an incident command center in the Colorado woods, don headlamps to locate victims, and communicate via radio to coordinate care. They triage wounded “patients” to determine who is most likely to survive, and figure out how best to evacuate them. Around 10 actors — often, course alumni — play the roles of passengers, replete with special-effects makeup that mimics cuts, frostbite, even broken bones.
“The rescue takes a lot of critical thinking, teamwork, and communication skills — much like working in a hospital. Students grow a great deal from the experience,” says Lara Phillips, MD, an SKMC clinical associate professor in emergency medicine and codirector of the course.
“They learn crucial skills, but some of the most important lessons they learn are around humility. There’s no room for embarrassment. You have to be able to acknowledge your limitations and ask for help to save lives.”
The rescue simulation follows two weeks of preparatory training at Colorado’s BOEC. Expert lecturers from across the country cover everything from altitude illness to antivenom treatment to knot-tying skills.
After the Colorado stint, the group heads to Utah for two weeks of hiking desert terrain and canoeing. There, simulations span rescuing a drowning victim to helping a woman in labor with only the resources at hand.
Sharing such intense experiences created powerful bonds among group members, says participant Macaluso. He particularly appreciated the opportunity to connect with the course’s leaders.
“Usually in medical school, discussions with attendings are pretty formal. Here, I got to know the instructors much more personally. I feel very comfortable reaching out to those instructors now.
“They also provided feedback that was highly personalized because they got to know me so well. They told me to keep my enthusiasm and my energy but said I should also learn to slow down and be a bit more deliberate. That advice was so valuable,” he says. “The whole experience was amazing.”
